DR Andrew j. HAYDUKE
Mastectomy is surgery to remove an entire breast to treat or prevent breast cancer. Most women who have a mastectomy have the option of having additional surgery to rebuild the shape of the removed breast. Balancing procedures on the opposite unaffected breast are also commonly performed.
Dr. Hayduke has been continuously performing breast reconstruction his entire career, ever since his earliest days in practice. Dr. Hayduke enjoys applying his artistic skills not just for cosmetic surgery clientele, but also for people afflicted with breast cancer and mastectomy. Breast cancer reconstruction has, and will continue to be, a major part of Dr. Hayduke’s practice of plastic surgery. Dr. Hayduke feels strongly that plastic surgeons should use their skills not just for cosmetic surgical issues, but also to help people who are truly in need.
Breast reconstructive surgery after mastectomy can be either immediate or delayed. With immediate reconstruction, a surgeon performs the first stage to rebuild the breast during the same operation as the original mastectomy.
With delayed reconstruction, the surgeon performs the first stage to rebuild the breast several months after the chest has healed from the mastectomy and after the woman has completed adjuvant chemotherapy and radiation.
Dr. Hayduke can rebuild breasts using implants (saline-filled or silicone-filled) or autologous tissue (that is, tissue moved from elsewhere in the patient’s own body). Most modern breast reconstructions performed today in the United States are immediate reconstructions with breast expanders and implants. This method is known as expander/implant breast reconstruction.
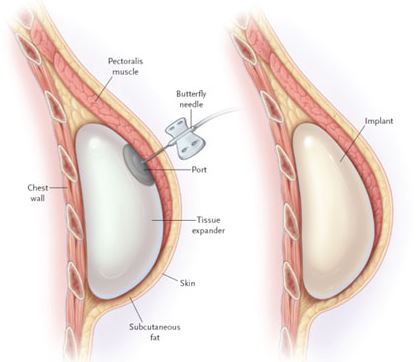
Breast expanders (temporary expandable implants) can be inserted underneath the skin and chest muscle that remain after a mastectomy, usually as part of a two-stage procedure.
|
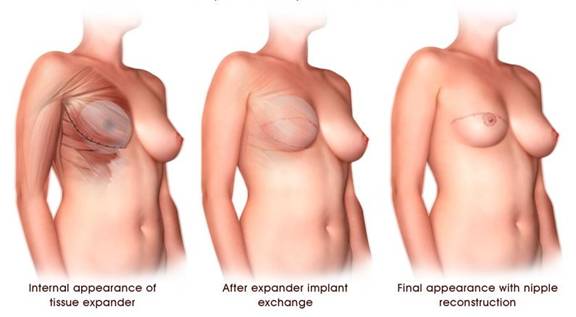
In the first stage, Dr. Hayduke places a device called a breast expander under the chest muscle. The breast expander is slowly filled with saline during subsequent visits to Dr. Hayduke after surgery (usually once a week for about 4 to 6 office expansion sessions). This allows gradual expansion of a breast pocket. In the second stage (stage 2), after the chest tissue has relaxed and healed enough (and a healthy pocket has been created), the expander is removed and replaced with a long term implant. Long term implants are either silicone or saline filled. The chest tissue is usually ready for exchanging the breast expander with and long term implant (stage 2) about 4 to 6 months after placement of the breast tissue expander.
Expanders can be placed as part of either immediate or delayed reconstructions. An optional third stage of breast reconstruction involves recreating a nipple on the reconstructed breast. This is known as nipple reconstruction.
|
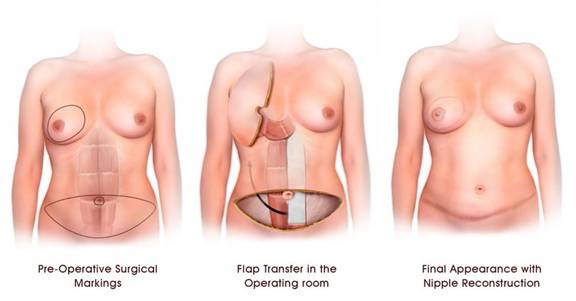
Although not the most common overall method of breast reconstruction, the most common method that actually uses your own tissues (autogenous) is the pedicled transverse rectus abdominus myocutaneous (TRAM) flap. In this approach, the entire rectus abdominus muscle is used to carry your lower abdominal skin and fat up into the mastectomy area. A breast shape is then created using your own lower abdominal fatty tissues. In order to transfer the flap to the chest, the muscle is tunneled underneath the upper abdominal skin. Since the patient’s own body tissue is utilized to create a breast, the result – in some cases, is a more natural breast reconstruction as compared to a pure implant reconstruction. A greater amount of droop or sagginess can usually be created with a TRAM breast reconstruction as compared to an expander/implant reconstruction. The scar on the abdomen is relatively low, and extends from hip to hip. The TRAM flap can be used for reconstructing one or both breasts. In a patient undergoing one sided reconstruction, the TRAM flap can potentially offer better symmetry than using just an implant – but that is not always the case. In some cases, an expander and/or implant is later placed underneath the TRAM reconstruction to give added size and roundness to the TRAM reconstructed breast, especially in those patients who had only a small amount of fatty tissue in their lower abdominal region.
|
While the benefit of the TRAM flap is a more natural looking (droopier) and more natural feeling breast as compare to pure implant reconstruction, the primary disadvantages of a TRAM relate to the abdominal wall donor site. These include potential abdominal wall weakness, permanent bulges, and permanent lower abdominal hernias. To decrease the chances of hernias and bulges, synthetic mesh is sometimes used when closing the abdomen. Bulges and hernias tend to occur in the zone where the rectus abdominus muscle was removed. In some cases, these abdominal bulges are large and unfortunately permanent.
The TRAM flap operation is more involved than pure expander/implant reconstruction. The length of surgery for a unilateral TRAM flap reconstruction is generally four to five hours. For bilateral reconstruction, it is approximately five to seven hours. The hospital stay is usually two to five days. The patient will have abdominal pain and tightness for several weeks, and it can often take several months to return to a full range of activity.
The latissimus dorsi (LD) flap is an old tried and proven method for breast reconstruction that was first utilized way back in the 1970’s. The latissimus dorsi flap is most commonly combined with a tissue expander or implant, to give the surgeon additional options and more control over the aesthetic appearance of the reconstructed breast. This flap provides a source of soft tissue that can help create a breast shape. The latissimus dorsi flap is also a great salvage procedure to repair and reconstruct the mastectomy site after serious radiation induced problems.
|
Many surgeons will resort to the use of an latissimus dorsi flap as a backup option if a patient has wound healing problems or soft tissue failure in the setting of an implant. The latissimus dorsi flap can also be used as a salvage procedure for patients who have had previous chest radiation, and are not candidates for other autogenous procedures. A large open wound on the chest wall is also an indication for an latissimus dorsi flap in patients that need chest wall reconstruction alone, without creation of a breast shape.
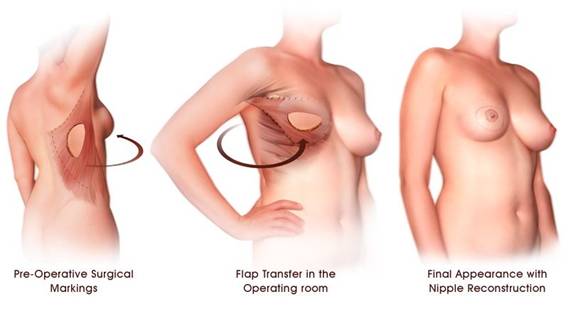
At the time of breast reconstruction, the latissimus dorsi muscle flap, with or without attached skin, is elevated off of the back and tunneled around to the front of the chest wall underneath a skin tunnel. The main blood vessels still remain attached to the body to ensure proper blood supply to the transposed flap. The LD flap provides soft tissue to allow complete coverage of an underlying implant.
The length of surgery for latissimus dorsi flap breast reconstruction is typically three to four hours, and requires one to two post-operative nights in a hospital. The initial recovery time is about three to four weeks. Depending on the patient, the scar from the LD flap donor site on the back can be placed diagonally or horizontally. A horizontal scar can sometimes be concealed underneath a wide bra strap. Patients generally have no major long-term physical limitations from taking the latissimus muscle. Activities of daily living and most exercise can be resumed without significant loss of proficiency.
Secondary procedures after an latissimus dorsi flap reconstruction can be done several months later. These may include expander implant exchange, adjustment procedures to improve breast symmetry, and nipple areola reconstruction. As with any type of reconstruction, if chemotherapy is needed, any additional surgery usually awaits completion of treatment. Such additional procedures are typically done as outpatient surgery with a rapid recovery.
You may be a candidate for latissimus dorsi flap reconstruction if you:
You are not an ideal candidate for LD flap reconstruction if you:
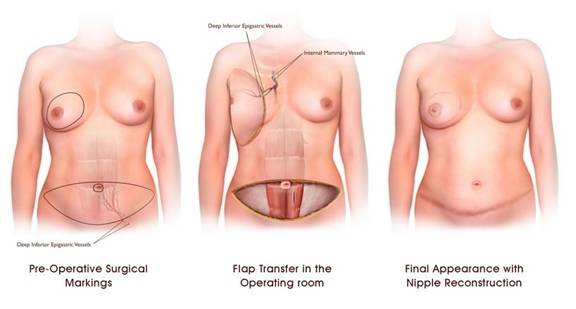
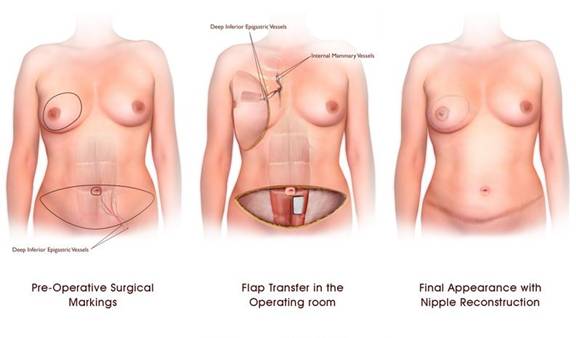
While the pedicled TRAM flap (not DIEP flap) is still the dominant flap reconstruction method in the United States for those who do not want expander/implant reconstruction, some plastic surgeons also offer microsurgical techniques, which provide women with another option to utilizing their own abdominal fatty tissue. In this complex procedure, the original artery and vein are cut to the transferred tissue and then sewn back together to another set of recipient artery and veins in the recipient location utilizing a large microscope. This complex option allows for achieving results with somewhat fewer donor site complications. No abdominal muscle is used. Nevertheless, this is a much longer procedure with potential for other major devastating complications such as total flap loss. Total flap loss means the entire transposed flap turns black and dies. The success rate in transferring tissue in this manner is reasonably good in the hands of surgeons who perform microsurgery regularly, in institutions with experience monitoring these flaps such as major universities rather than private community hospitals. If blood vessel thrombosis (clotting) occurs in the transplanted flap, urgent re-operation is required for flap salvage, or total flap loss (total flap tissue death) will result. Before proceeding with a DIEP flap, the patient should ask their plastic surgeon as to their volume of microsurgery experience, and their overall rate of recent success. They should ask the surgeon how many DIEP flaps have they performed within the last 12 months. If this complex microsurgery is chosen, usually a major university who performs a large volume of DIEP flap reconstruction would be the smartest choice. This requires careful research and usually significant travel on the part of the patient.
|
Another method of complex microvasular breast reconstruction is called the “TRAM free flap”. The TRAM free flap is similar to the DIEP flap in that this type of flap is also based on the deep inferior epigastric vessels. In the TRAM free flap, the lower abdominal skin and fat is removed along with a small portion of the rectus muscle. The portion of muscle removed carries these blood vessels with the flap.
Using a microscope, the TRAM free flap can then be transplanted to a recipient set of blood vessels on the chest wall. As with the DIEP or SIEA flaps, the tissue is used to create a breast shape without having to be tunneled under the skin (as in the pedicled TRAM flap).
|
Creating the nipple is one of the last components to making your breast reconstruction complete. There have been numerous approaches to nipple reconstruction over the last several decades, and with several options available, surgeons can utilize whichever method is most suitable for their patients. There is no one absolute best method of nipple reconstruction for all patients. Some patients are comfortable without having a nipple, and do not wish to have further surgery. Others choose the non-surgical option of tattooing without actual central nipple protrusion reconstruction. This allows color pigmentation to simulate the nipple areola without the contour or protrusion of an actual central nipple. Still, the reconstruction of the nipple helps to put the finishing touches on the new breast after a long journey in reconstruction.
|
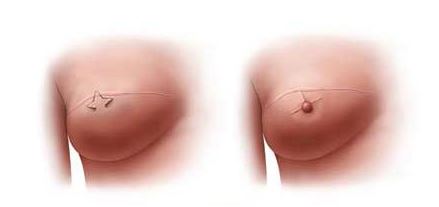
In modern approaches to nipple reconstruction, the nipple mound protrusion is created from skin taken as a local flap on the reconstructed breast itself. Various local flaps have been described, including the Star flap, the C-V flap and the Skate flap. Regardless of which approach your surgeon chooses, the outcome will be a slightly protruding nipple. Two to three months later, the areola can be either tattooed around the nipple (most commonly), or the areola can be reconstructed with a more complex skin graft taken from elsewhere on the body.
The finishing touch to breast reconstruction is having your nipple areola tattooed. This is done by Dr. Hayduke himself in his office. Tattooing is a simple, fast procedure. As with any tattoo, the pigment will fade in time. Getting the right shade of color may require more than one tattoo procedure. If you have had a breast implant and regained some breast skin sensation, Dr. Hayduke will give you an injection of local anesthetic. Most patients with flap reconstruction have very little sensation. After drawing the outline of the areola and confirming the design with you, Dr. Hayduke will place the tattooing instrument against your reconstructed breast. You may feel a pushing and vibrating sensation, as many ultra fine needles transfer pigment into the deep layers of your skin. Since local anesthetic was already injected, it should be completely painless at this point.
It is important to consider the opposite breast when planning your reconstruction. While some women choose to leave the healthy breast untouched, many want to achieve better symmetry with the newly reconstructed breast. Depending on the needs of the patient, symmetry may be achieved with a breast reduction, breast lift, or breast enlargement with an implant. The timing of these procedures will vary depending on what other treatments you may need.
The approach to surgery on the opposite breast will vary depending on the type of reconstruction you have chosen and your personal anatomy (weight). For patients with flap reconstruction, the opposite breast may be operated on during the second stage of surgery when the flap is revised and the nipple areola reconstructed. For patients with expander implant reconstruction, the opposite breast can be operated on when the expander is exchanged for the final implant, or it may require a separate third surgery for best esthetic results. Because implants tend to be round in shape, having an implant placed into the opposite non-mastectomy breast may offer better symmetry with an implant reconstructed mastectomy site. The nipple areola will then be reconstructed at a later time, once the final implant and the opposite breast have all settled and healed.
Every woman having a mastectomy should be aware of this act. The Women’s Health and Cancer Rights Act (WHCRA) contains important protections for women with breast cancer who choose to have breast reconstruction after a mastectomy. It was signed into law on October 21, 1998. The US Departments of Labor and Health and Human Services have oversight of this law.
WHCRA:
Under WHCRA, mastectomy benefits must include coverage for:
Mastectomy health plan benefits may have a yearly deductible and coinsurance (a form of insurance in which health costs are insured for less than the full amount and the patient is responsible for the difference) but they must be like those established for other benefits under the plan or coverage.
The WHCRA will not allow: